From MIT Technology Review: "Are Young Athletes Risking Brain Damage?"
And with the increasing awareness of concussion injuries, comes a rise in bogus (or marginal) services.
The blog of Freedom and Individual Rights in Medicine (FIRM)
Tuesday, December 22, 2015
Monday, December 21, 2015

Friday, December 18, 2015
Politics and Health
This New York Times column by Dr. Aaron Carroll acknowledges an important truth: "Even in Basic Health Decisions, You Can’t Screen Out Politics".
Whenever people expect "somebody else" to pay for their health care, then inevitably "somebody else" will decide what care they will (or will not) receive.
This is also why I support health reforms that allow patients to control as much of their own health spending as possible (such as Health Savings Accounts, direct pay primary care, and catastrophic-only insurance with as few mandated benefits as possible.)
Whenever people expect "somebody else" to pay for their health care, then inevitably "somebody else" will decide what care they will (or will not) receive.
This is also why I support health reforms that allow patients to control as much of their own health spending as possible (such as Health Savings Accounts, direct pay primary care, and catastrophic-only insurance with as few mandated benefits as possible.)
Tuesday, December 15, 2015
Hsieh Forbes Column: Are Mandatory Electronic Medical Records Causing Doctor Burnout?
I've expanded my latest blog post into a new Forbes column: "Are Mandatory Electronic Medical Records Causing Doctor Burnout?"
In this piece, I discuss why both doctors and patients are frustrated with electronic medical records (EMRs), drawing upon good reporting from the Chicago Tribune and the Wall Street Journal. I also discuss some ways patients can act to protect the quality of their health care, despite the problems caused by the EMRs.
Thanks to Dr. Matthew Bowdish for alerting me to the WSJ piece.
Bonus: I managed to violate Betteridge's Law of Headlines!

In this piece, I discuss why both doctors and patients are frustrated with electronic medical records (EMRs), drawing upon good reporting from the Chicago Tribune and the Wall Street Journal. I also discuss some ways patients can act to protect the quality of their health care, despite the problems caused by the EMRs.
Thanks to Dr. Matthew Bowdish for alerting me to the WSJ piece.
Bonus: I managed to violate Betteridge's Law of Headlines!

Mandatory Electronic Records and Doctor Burnout
Detailed piece in the 12/12/2015 Chicago Tribune: "Beleaguered by electronic record mandates, some doctors burning out".
One excerpt:
Imagine if the government mandated electronic accounting software for all small businesses for billing and inventory, regardless of whether or not a particular business found it worthwhile. Or if the government mandated universal smartphone ownership, whether or not an individual needed those capabilities. Such mandates would have a hugely distorting effect on the quality and usability of the product.
Image below from the article: "Dr. Niva Lubin-Johnson, an internist, walks with her laptop to see a patient Dec. 8, 2015, at her practice in Chicago's Chatham neighborhood. She is unhappy with federal requirements for electronic health records. (Zbigniew Bzdak / Chicago Tribune)"

One excerpt:
There are so many boxes to click through, she [Dr. Niva Lubin-Johnson] wonders whether she spends more time with her patients or with her computer. She's had to cut back from seeing four patients an hour to three so she doesn't feel overwhelmed. When she does examine patients, she also spends much of her time on her laptop, filling out dozens of electronic forms mandated by law.The concept of electronic medical records is good. But these were never adopted in an organic fashion by physicians and hospitals choosing in a free market which systems to purchase, based the feature sets that helped them and their patients. Rather, they were rammed down doctors' throats via government carrots-and-sticks. Vendors essentially had a captive audience.
"Is this really helping us with patient care? The answer is no. We're just checking off boxes, sending in a report," said Lubin-Johnson, 58.
It's getting to the point where she is looking forward to retiring. It's a thought she rarely entertained before the federal government began requiring physicians to use an elaborate — or maddening and onerous — system of electronic health records four years ago or face penalties worth tens of thousands of dollars in lower Medicare reimbursements.
Imagine if the government mandated electronic accounting software for all small businesses for billing and inventory, regardless of whether or not a particular business found it worthwhile. Or if the government mandated universal smartphone ownership, whether or not an individual needed those capabilities. Such mandates would have a hugely distorting effect on the quality and usability of the product.
Image below from the article: "Dr. Niva Lubin-Johnson, an internist, walks with her laptop to see a patient Dec. 8, 2015, at her practice in Chicago's Chatham neighborhood. She is unhappy with federal requirements for electronic health records. (Zbigniew Bzdak / Chicago Tribune)"
Thursday, December 3, 2015
They Did WHAT To Revive People In The 18th Century ?!?
From Neatorama: "This Emergency Enema Kit Was the Defibrillator of the 18th Century".
I am so very, very, very, thankful that we've progressed past this point:

I am so very, very, very, thankful that we've progressed past this point:
According to Eighteenth Century British medicine, that it was possible to revive a person who had stopped breathing by blowing tobacco smoke up his rectum. Emergency enema kits like these were the defibrillators of the day: essential lifesaving tools designed by medical professionals. Ella Morton of Atlas Obscura writes:I'm surprised this hasn't been on an episode of House, MD.
Cardiopulmonary resuscitation, or CPR, was still centuries away from common usage. Instead of pumping the chest or giving mouth-to-mouth to a drowning victim—a practice that prominent British doctor William Hunter called "vulgar" in 1776—rescuers employed a variety of other dubious methods when attempting to revive those with waterlogged lungs. Rubbing the skin, inflating the lungs via a tube inserted into the trachea, and bloodletting were among the approaches. The most creative technique, however, was rectal tobacco insufflation—piping smoke into the unconscious person’s intestines via a bellows inserted in the anus.Occasionally the process worked. The medical journal The Lancet repeats a story from 1746:
A man's wife was pulled from the water apparently dead. Amid much conflicting advice, a passing sailor proffered his pipe and instructed the husband to insert the stem into his wife's rectum, cover the bowl with a piece of perforated paper, and ‘blow hard.’ Miraculously, the woman revived.
Wednesday, December 2, 2015
Your Doctor Doesn't Want to Hear About Your Fitness-Tracker Data
Basically, it's the medical version of TMI -- "Your Doctor Doesn't Want to Hear About Your Fitness-Tracker Data":

Wearable producers such as Apple, Fitbit, and Pebble will ship more than 76 million of the devices by the end of the year, according to market research firm IDC. Some doctors and researchers, however, remain unimpressed, They question the value of the particular metrics tracked, as well as the validity of the deluge of data these gadgets produce...
Monday, November 30, 2015
Hsieh Forbes Column: Why You Want Your Doctor To Be Wrong (Sometimes)
My latest Forbes piece is now out, "Why You Want Your Doctor To Be Wrong (Sometimes)".
Here is the opening:
For more details, read the full text of "Why You Want Your Doctor To Be Wrong (Sometimes)".
And my personal favorite example of Type 1 vs. Type 2 errors is below:

Here is the opening:
“Mommy, my tummy really hurts!”I discuss Type 1 vs. Type 2 errors, why they are important, and why certain kinds of diagnostic errors are not merely unavoidable but (in the right context) desirable.
Your 7-year old daughter wakes you up in the middle of the night, doubled over in pain. You take her to the local ER. The on-call surgeon, Dr. Smith, performs a thorough physical exam, reviews the test results, informs you that she has appendicitis, and says she needs surgery right away. You sign the consent forms, and he whisks her off to the OR. An hour later, Dr. Smith comes back and says, “I’m sorry. We removed her appendix, but it turned out to be normal. She didn’t have appendicitis, just a severe case of gastroenteritis or ‘stomach flu’.”
Should you be relieved or angry? Did Dr. Smith make a mistake? Did he perform an unnecessary operation?...
For more details, read the full text of "Why You Want Your Doctor To Be Wrong (Sometimes)".
And my personal favorite example of Type 1 vs. Type 2 errors is below:
Monday, November 23, 2015
Thursday, November 19, 2015
When Unethical Medical Experiments Bear Fruit
I'm not a utilitarian, and the medical experiments described below were truly appalling.
But there is some informative medical history in this piece: "These medical experiments were horrible, unethical — and useful".
People can debate some of the fine points of the current system of IRB (Institutional Review Board) approval and informed consent for medical experiments. But the current system is far better than what has occurred in the past.

But there is some informative medical history in this piece: "These medical experiments were horrible, unethical — and useful".
People can debate some of the fine points of the current system of IRB (Institutional Review Board) approval and informed consent for medical experiments. But the current system is far better than what has occurred in the past.
Tuesday, November 17, 2015
Short Story: SMOD 2016
I'm exercising blogger's privilege to post something totally unrelated to health care policy.
Here's my latest short story, "SMOD 2016" (400 words). FYI, it's a little dark, in the spirit of Frederic Brown.
Here is the opening:
Read the rest at: "SMOD 2016".
["Asteroid Belt", image courtesy Wikipedia.]

Here's my latest short story, "SMOD 2016" (400 words). FYI, it's a little dark, in the spirit of Frederic Brown.
Here is the opening:
SMOD 2016
A short story by Paul Hsieh
"So, basically you're saying that humanity should be extinct by now." MIT astrophysics professor Linda Tsang furrowed her brow.
"Yes, many times over," replied statistics professor Max Wendt. "Based on the new telescope data you provided me about the asteroid belt, the Earth should have been struck by a 'Dinosaur Killer' rock at least 5 or 6 times in the past 10,000 years."
"So, why haven't we?" asked Tsang.
"Well, there are a few possibilities," said Wendt...
Read the rest at: "SMOD 2016".
["Asteroid Belt", image courtesy Wikipedia.]

Monday, November 16, 2015
The Inadequacy of 15-Minute Medicine
In the Washington Post, Dr. Michael Stein writes: "When medical care is delivered in 15-minute doses, there's not much time for caring".
Dr. Stein's bottom line:
One excerpt:

Dr. Stein's bottom line:
My job, in its barest 15-minute form, is to separate the serious possibilities from the less serious, offer a diagnosis and an explanation, recommend any additional testing and list the possible courses of action. But a hurried, task-oriented approach doesn’t accommodate the meandering, overlapping, widening issues of patients. It undermines kindness. And it prevents doctors from being what our patients hope we will be when they walk in: unrushed explorers on the lookout for the next discovery.Fortunately, patients and doctors can avoid these problems through a "direct pay" or "concierge" model, as discussed in my earlier Forbes piece, "Is Concierge Medicine The Correct Choice For You?". Doctors can take the time to give the patients' issues the attention they need.
One excerpt:
In response to this frustrating situation, more doctors are seeking an alternative practice model. They are establishing “concierge” or “direct pay” practices, where patients pay a monthly or annual fee for enhanced services, including same day appointments, 24/7 access to their doctor, e-mail consultations, and longer appointment times. Instead of the usual rushed 10-15 minute appointments, these doctors typically offer 45-60 minute visits allowing them to really delve into their patients’ problems and craft individualized treatment and prevention plans.(Washington Post link via Dr. Matthew Bowdish.)
The Indianapolis Business Journal described how concierge medicine helped patient Dale Sventeck. Sventeck suffered from a “frozen shoulder” which severely limited his range of motion. Most doctors he saw simply wanted to schedule him for an MRI study and surgery. But concierge physician Kevin Logan was able to take the time to diagnose that Sventeck’s problem was caused by the mercury in his dental fillings. Dr. Logan advised Sventeck to remove the fillings. One month later, his shoulder was back to normal.

Thursday, November 5, 2015
Sissel Lawsuit Update
Matt Sissel has an OpEd in the 11/3/2015 Washington Times on his anti-Obamacare lawsuit: "Taking a stand against Obamacare".
Sissel is being represented by Timothy Sandefur of the Pacific Legal Foundation (PLF). For more details, see the PLF page on the case.
I wish them both success in their fight for individual rights!

Sissel is being represented by Timothy Sandefur of the Pacific Legal Foundation (PLF). For more details, see the PLF page on the case.
I wish them both success in their fight for individual rights!
Monday, November 2, 2015
NEJM On Peer Review Fraud
New England Journal of Medicine: "Peer-Review Fraud -- Hacking the Scientific Publication Process".
Fraudulent reviews on Amazon or Yelp are bad enough. Fraudulent peer review in science and medicine could be very, very dangerous to patients.
Fraudulent reviews on Amazon or Yelp are bad enough. Fraudulent peer review in science and medicine could be very, very dangerous to patients.
Wednesday, October 28, 2015
Washington Post Vs. Paternalistic Breast Cancer Guidelines
Washington Post editor Marisa Bellack speaks out against paternalistic mammography guidelines in her editorial, "Don't worry your pretty little head about breast cancer".
She notes that "anxiety" is being increasingly invoked as a (bad) reason to limit screening mammography, especially for women between ages 40-49:
See also this related Washington Post piece, "Why this Harvard radiologist still recommends women get mammograms at age 40".
(Link via Dr. Evan Madianos.)
She notes that "anxiety" is being increasingly invoked as a (bad) reason to limit screening mammography, especially for women between ages 40-49:
And yet, there was a 19th-century echo in the American Cancer Society’s announcement this past week of revised guidelines for breast cancer screening. Whereas anxiety was once a reason for aggressive medical intervention, it is now invoked to avoid intervention — an argument that is both patronizing and unscientific. There may be good reasons for women in their early 40s to forgo regular mammograms, but this isn’t one of them.For more details, read the full text of "Don't worry your pretty little head about breast cancer".
A reference to anxiety appears in the very first paragraph of the harms-and-benefits analysis commissioned by the cancer society: While early screening “reduces breast cancer mortality, there are a number of potential harms, including false-positive results, which result in both unnecessary biopsies and increased distress and anxiety related to a possible diagnosis of cancer.”
But the idea that anxiety is a major harm doesn’t have much scientific support...
There will always be uncertainty in cancer screening. And that uncertainty understandably fuels anxiety. But most false-positive mammograms are quickly resolved by additional imaging. Among the cases that progress to biopsies, 9 out of 10 show no sign of cancer. And even when there is a breast cancer diagnosis, that’s not equivalent to a death sentence. Doctors should be able to respond to anxiety rationally, putting fears in context and expediting follow-up testing and results to limit what can be an agonizing wait.
See also this related Washington Post piece, "Why this Harvard radiologist still recommends women get mammograms at age 40".
(Link via Dr. Evan Madianos.)
Monday, October 26, 2015
Hsieh Forbes Column On Doctor 'Report Cards' And Unintended Consequences
My latest Forbes piece is now out, "Doctor 'Report Cards' May Be Hazardous To Your Health".
I discuss the rise of physician "report cards" for heart surgeons and other advanced surgical specialties, as well as some of the unintended consequences these report cards can create for patients.
One take home point from my piece:
Various private rating systems will be a mixed bag, each with their own strengths and flaws. I personally think all such ratings will have flaws that patients need to know about, which is one point of my article. Fortunately, patients can listen to (or ignore) those ratings as long as they remain private.
In contrast, government rating system will be very easily captured by those with agendas that don't necessarily align with patient interests (such as cost containment), and that's where we can potentially see big trouble.
For more details, read the full text of "Doctor 'Report Cards' May Be Hazardous To Your Health".
I also recommend a related article by Dr. Saurabh "Harry" Jha, "When a bad surgeon is the one you want: ProPublica introduces a paradox".

I discuss the rise of physician "report cards" for heart surgeons and other advanced surgical specialties, as well as some of the unintended consequences these report cards can create for patients.
One take home point from my piece:
The report cards can tell you how many patients died under a particular surgeon’s care. But they can’t tell you how many of those patients would have died without surgery. And more importantly, the report cards can’t tell you how many of those same patients would have died if treated by a different surgeon — because each surgeon gets to choose which patients he or she will operate on.I also cover other ways patients can find a good surgeon, in addition to these "report cards".
The goal of recognizing good doctors is laudable. But the proposed “report cards” have serious limitations. Patients looking for a good surgeon should consider these report cards as merely one data point among many — and not necessarily the most reliable.
Various private rating systems will be a mixed bag, each with their own strengths and flaws. I personally think all such ratings will have flaws that patients need to know about, which is one point of my article. Fortunately, patients can listen to (or ignore) those ratings as long as they remain private.
In contrast, government rating system will be very easily captured by those with agendas that don't necessarily align with patient interests (such as cost containment), and that's where we can potentially see big trouble.
For more details, read the full text of "Doctor 'Report Cards' May Be Hazardous To Your Health".
I also recommend a related article by Dr. Saurabh "Harry" Jha, "When a bad surgeon is the one you want: ProPublica introduces a paradox".

Sunday, October 25, 2015

Saturday, October 24, 2015
Ebola Quarantine Lawsuit
Doug Mataconis discusses: "Nurse Kaci Hickcox Sues Chris Christie For Civil Liberties Violations During Ebola Quarantine".
This is some legal fallout from last year's big Ebola scare, in which many people were calling for restrictions on people coming to the US from affected areas in Africa.
From Mataconis' blog post:
The key issue in this case is whether someone who displayed no symptoms and was supposedly not at risk of transmitting the disease to others posed such an "objective threat".

This is some legal fallout from last year's big Ebola scare, in which many people were calling for restrictions on people coming to the US from affected areas in Africa.
From Mataconis' blog post:
[Kaci Hickcox] was detained at Newark Airport after arriving home from West Africa and not allowed to continue on to her connecting flight. Instead, she was taken into custody and detained in a tent outside a hospital in Newark, New Jersey before being allowed to return home to Maine.I fully agree with the principle that the government has the legitimate authority to quarantine people who carry a deadly infectious disease -- or who pose an objective threat of such -- based on best reasonable medical knowledge.
Once in Maine, that state’s Republican Governor Paul LePage, who just happened to be running for re-election, attempted to impose severe restrictions on Hickox’s liberty notwithstanding the fact that she displayed absolutely no symptoms of having the Ebola virus and that asymptomatic patients are not contagious.
Governor LePage’s efforts were derailed by a Maine State Court Judge, who limited the requirements placed on Hickox to keeping local health authorities informed of her condition and location during the incubation period for the disease.
Now, Hickcox has filed a lawsuit alleging that Christie and other government authorities violated her civil liberties...
The key issue in this case is whether someone who displayed no symptoms and was supposedly not at risk of transmitting the disease to others posed such an "objective threat".
Friday, October 23, 2015
In Defense Of Old Mammography Guidelines
In response to new mammography guidelines from the American Cancer Society, the Washington Post covered the controversy in their 10/20/2015 piece: "Why this Harvard radiologist still recommends women get mammograms at age 40".
They interviewed Dr. Daniel Kopans, professor of radiology at Harvard Medical School and a radiologist at Massachusetts General Hospital. Dr. Kopans discussed why age 40 should be retained as a better threshold than 50 for screening, as well as issues of overdiagnosis and insurance coverage.
Read the full text for more information.

They interviewed Dr. Daniel Kopans, professor of radiology at Harvard Medical School and a radiologist at Massachusetts General Hospital. Dr. Kopans discussed why age 40 should be retained as a better threshold than 50 for screening, as well as issues of overdiagnosis and insurance coverage.
Read the full text for more information.

Wednesday, October 21, 2015
The Flip Side of Shopping Solely By Price
Health care reporter Sarah Kliff decided to go with the least expensive MRI scan to check for a stress fracture in her foot.
Her conclusion: "I didn't think I was making any trade-off when I chose a cheaper MRI. Now I know that isn't true."
(See earlier piece, "NPR: Pay Patients, Save Money".)
/cdn0.vox-cdn.com/uploads/chorus_asset/file/3563812/464795478.0.jpg)
Her conclusion: "I didn't think I was making any trade-off when I chose a cheaper MRI. Now I know that isn't true."
(See earlier piece, "NPR: Pay Patients, Save Money".)
Monday, October 19, 2015
Get Out of Obamacare
The Atlantic lists "All the Ways to Get Out of Obamacare".
Lots of government fine print. (Via Dr. Megan Edison.)
Lots of government fine print. (Via Dr. Megan Edison.)
Wednesday, October 14, 2015
NPR: Pay Patients, Save Money
NPR's Planet Money podcast discusses a novel program to help patients save money on health care by cutting them in for a piece of the savings: "Pay Patients, Save Money".
Although not a fully market-based mechanism, it does show that patients can respond to incentive when they have "skin in the game".
For similar reasons, I support Health Savings Accounts and other market-oriented mechanisms to give patients more flexibility and control over their health spending.

Although not a fully market-based mechanism, it does show that patients can respond to incentive when they have "skin in the game".
For similar reasons, I support Health Savings Accounts and other market-oriented mechanisms to give patients more flexibility and control over their health spending.
Monday, October 12, 2015
Wednesday, September 30, 2015
Doctors Leaving The UK
The Economist discusses the growing problem of unhappy UK physicians, "Some junior doctors consider a strike, while others pack their bags".
One possible "canary in the coal mine" indicator:
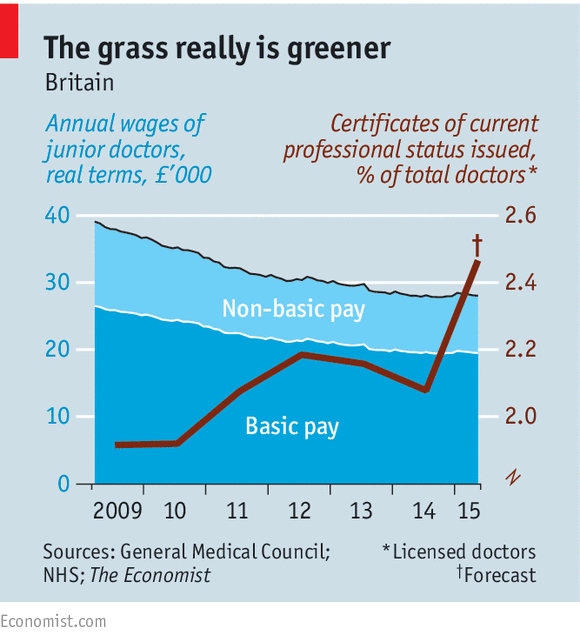
One possible "canary in the coal mine" indicator:
Like workers in any public service, doctors always say that morale has never been lower. But this time many are threatening to vote with their feet and practise overseas. Normally the General Medical Council, which regulates the profession, gets 20-25 requests a day for certificates of professional status, which make it easier to work abroad. From September 16th-18th it received a staggering 1,644 requests.
Monday, September 28, 2015
Hsieh Forbes Column on Bad Science Reporting
My latest Forbes piece is now out: "How To Protect Yourself Against Bad Science Reporting".
I discuss some sources of error and bias that lead to bad science reporting, including:
For more details, read the full text of "How To Protect Yourself Against Bad Science Reporting".

I discuss some sources of error and bias that lead to bad science reporting, including:
1) Many publicly reported science results are still provisionalThis latest piece is relatively non-political. But it is uncompromisingly pro-bacon.
2) Beware of sloppy statistics
3) Beware of the bias towards positive dramatic results
For more details, read the full text of "How To Protect Yourself Against Bad Science Reporting".
Thursday, September 24, 2015
Preventing Medical Errors
Medical errors will happen. As Arlene Weintraub notes in Forbes, "Doctors Are Screwing Up Diagnoses -- And Patients Should Speak Out".
An excerpt:
And overall, patients should treat physicians as advisors -- but not infallible authorities.
An excerpt:
The authors of the IOM report identify several possible methods for encouraging patients to get more involved in their diagnoses. First, they suggest that the act of diagnosis should no longer be treated as a solitary task that takes place mostly inside a single clinician’s brain—but rather as a team effort that includes patients and their families. To achieve that, the authors admit, the entire culture of the healthcare system needs to change to one that welcomes patient feedback...I personally think that patient should obtain their own personal copies any important medical records (including radiology studies on CT, pathology reports, etc.) in case they wish to review them at home or in consultation with an independent physician.
And overall, patients should treat physicians as advisors -- but not infallible authorities.
Tuesday, September 22, 2015
Adalja on Pyrimethamine and The Market
Dr. Amesh Adalja discusses "Pyrimethamine and the Market". An excerpt:

While I have no understanding of how the new price was determined, it will eventually have to withstand the scrutiny of the market. If the price is set higher than the market will bear, because it is no longer under patent, other manufacturers will enter the market lowering prices. Ideally this would happen near instantaneously but, because of legislative barriers to entry, which include a multi-step approval process, it will take some time. Better alternatives to the current regimen may also appear in time as well.
Overall, however, infectious disease products have become less attractive to pharmaceutical companies and this, at root, is why we are left with just one manufacturer for many important non-patented products. The disincentives to enter this market are myriad and the ultimate answer to this scenario is not more intervention but to remove artificial barriers to entry, inviting the appearance of competitors in the market...
Monday, September 21, 2015
Speed Bumps And Appendicitis
From the British Medical Journal, "Pain over speed bumps in diagnosis of acute appendicitis: diagnostic accuracy study":

Which indicates how poor a clinical exam is for diagnosing appendicitis. And why the CT scanner has made such an important difference. (BMJ link via Slate.)

Our results confirm that an increase in pain while travelling over speed bumps is associated with an increased likelihood of acute appendicitis. Absence of pain over speed bumps is associated with a significantly decreased likelihood of appendicitis. Although the specificity was relatively low, as a diagnostic variable pain over speed bumps compared favourably with other features commonly used in diagnostic assessment, with a better sensitivity and negative likelihood ratio than all other features assessed.And some comparison data with other clinical signs (Table 2 in the article, click on image to see full-sized version):
Moreover, some patients who were “speed bump positive” but did not have appendicitis had other important abdominal diagnoses, such as a ruptured ovarian cyst, diverticulitis, or pelvic inflammatory disease...

Which indicates how poor a clinical exam is for diagnosing appendicitis. And why the CT scanner has made such an important difference. (BMJ link via Slate.)
Wednesday, September 16, 2015
More Anti-MOC Backlash
Kurt Eichenwald at Newsweek has an update: "To the Barricades! The Doctor’s Revolt Against ABIM is Underway".
He discusses the growing backlash against the "Maintenance of Certification" (MOC) requirements by the American Board of Internal Medicine (ABIM). In theory, a private agency that certifies that doctors are keeping up on important clinical knowledge is good. But his series of articles on the ABIM's process shows serious problem with the specific methods chosen.
From the article:
Let's hope the ABIM learns from their example.
And kudos to Kurt Eichenwald for continuing to report on this developing issue.
(Link via Dr. Megan Edison and Dr. Matthew Bowdish.)

He discusses the growing backlash against the "Maintenance of Certification" (MOC) requirements by the American Board of Internal Medicine (ABIM). In theory, a private agency that certifies that doctors are keeping up on important clinical knowledge is good. But his series of articles on the ABIM's process shows serious problem with the specific methods chosen.
From the article:
Dr. Jones can’t manage his practice, care for his family and study for the certification exams administered by the American Board of Internal Medicine. The tests purportedly insure doctors’ competence, but, like many physicians, Dr. Jones says the questions often have nothing to with what he sees in his practice and are little more than a game of medical Trivial Pursuit. Dr. Jones can’t afford the thousands of dollars for study guides and classes to learn obscure, often irrelevant information, and has no time to review the material every night for months. He failed the test, so his hospital will no longer allow him to admit patients because he couldn’t answer questions about diseases he will never encounter....The article also describes how other specialties (such as the anesthesiologists certification board) are adopting other methods to ensure physician quality through tests and quizzes that are more relevant to clinical practice.
This medical protection racket has made millionaires of ABIM top officers, financed a ritzy condominium, limousines and first-class travel, all while sucking huge sums of cash out of the health care system. But now, after decades of unchecked rule by ABIM, cracks are appearing in the organization’s facade of power. Thousands of doctors began a widespread revolt months ago and, in the last few weeks, evidence that their efforts are succeeding has started rolling in...
[A recent study in the Annals of Internal Medicine] concluded that internists incur an average of $23,607 in MOC costs over 10 years—with doctors who specialize in cancers and blood diseases out $40,495. All told, the study concluded, MOC will suck $5.7 billion out of the health care system over 10 years, including $5.1 billion in time costs (resulting from 32.7 million physician-hours spent on MOC) and $561 million in testing costs. And remember—all that time and expense is for a program that has not been proven to accomplish anything.
Let's hope the ABIM learns from their example.
And kudos to Kurt Eichenwald for continuing to report on this developing issue.
(Link via Dr. Megan Edison and Dr. Matthew Bowdish.)
Thursday, September 10, 2015
Quick Links: Anti-MOC Backlash, Google, Apple
The Washington Post reports how anti-MOC (Maintenance of Certification) forces are gaining momentum, "Doctors' group will scrap 10-year re-certification exam":
Time magazine discusses the new Google health initiative in "Here's What 6 Doctors Really Think of Dr. Google". Personally, I think this will a tremendous value for patients and doctors in the long run.
The new Apple iPad Pro could help physicians better communicate important anatomy concepts to patients. The discussion of medical applications starts at 42:00 in this video. (Link via Ari Armstrong.)

The professional group that represents anesthesiologists will become the first medical board to scrap a widely criticized test that most physicians take every 10 years to demonstrate that they are up to date in their specialties, officials said Wednesday.(For more background on the MOC controversy, see these earlier Newsweek pieces "The Ugly Civil War in American Medicine" and "A Certified Medical Controversy".)
Time magazine discusses the new Google health initiative in "Here's What 6 Doctors Really Think of Dr. Google". Personally, I think this will a tremendous value for patients and doctors in the long run.
The new Apple iPad Pro could help physicians better communicate important anatomy concepts to patients. The discussion of medical applications starts at 42:00 in this video. (Link via Ari Armstrong.)

Tuesday, September 1, 2015
Market for "Perfect Poop"
From CNN: "One man's poop is another's medicine".
Donors who qualify can earn $40 per sample of "perfect poop", to be used for fecal transplantation to treat patients with C. difficile infection:
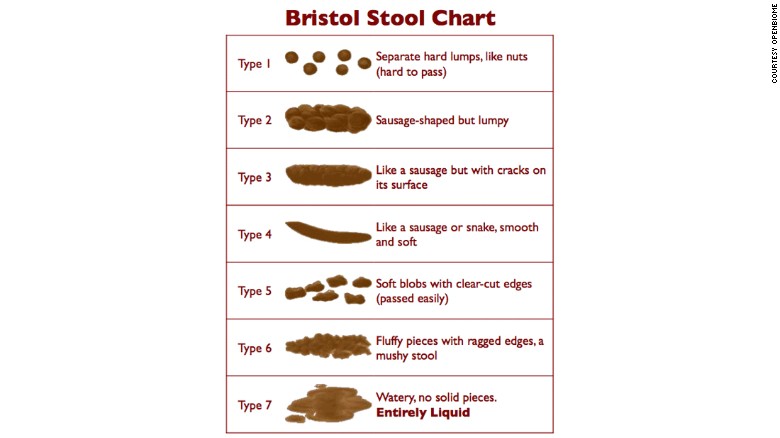
The poop also has to have the acceptable texture, either types 3, 4, or 5, on the Bristol Stool Chart:
Donors who qualify can earn $40 per sample of "perfect poop", to be used for fecal transplantation to treat patients with C. difficile infection:
Prospective donors are told, "It's easier to get into MIT and Harvard than it is to get enrolled as one of our donors."To donate, Eric had to pass a 109-point clinical assessment. There is a laundry list of factors that would disqualify a donor: obesity, illicit drug use, antibiotic use, travel to regions with high risk of contracting diseases, even recent tattoos. His stools and blood also had to clear a battery of laboratory screenings to make sure he didn't have any infections.After all that screening, only 3% of prospective donors are healthy enough to give. "I had no idea," he says about his poop. "It turns out that it's fairly close to perfect."And that, unlike most people's poop, makes Eric's worth money. OpenBiome pays its 22 active donors $40 per sample. They're encouraged to donate often, every day if they can. Eric has earned about $1,000.
The poop also has to have the acceptable texture, either types 3, 4, or 5, on the Bristol Stool Chart:
Monday, August 31, 2015
Hsieh Forbes Column: The Positive Value of Negative Drug Trials
My latest Forbes piece is now out: "The Positive Value of Negative Drug Trials".
I discuss the unfortunate bias against publishing "negative" scientific results that show a drug doesn't have much clinical benefit, and why it's in the self-interest of drug companies to still report these.
In particular, I highlighted two interesting facts:
For more details, read the full text of "The Positive Value of Negative Drug Trials".

("Fluoxetine 20 mg capsules" by Tom Varco - Own work. Licensed under CC BY-SA 3.0 via Commons; source: Wikipedia.)
I discuss the unfortunate bias against publishing "negative" scientific results that show a drug doesn't have much clinical benefit, and why it's in the self-interest of drug companies to still report these.
In particular, I highlighted two interesting facts:
1) Most drug trial results are still not being reported to a central registry.Fortunately, free market incentives are driving more drug companies towards full disclosure of both positive and negative study results -- which will benefit patients.
2) Negative results funded by private industry (e.g., pharmaceutical companies) are more likely to be reported than from government-funded research.
For more details, read the full text of "The Positive Value of Negative Drug Trials".
("Fluoxetine 20 mg capsules" by Tom Varco - Own work. Licensed under CC BY-SA 3.0 via Commons; source: Wikipedia.)
Monday, August 24, 2015
New Push To Regulate Personal Trainers
An interesting (but not very surprising) consequence of ObamaCare -- a new push to regulate personal trainers. This is gaining traction in the District of Columbia, but expected to spread soon to all 50 states as well.
From the 8/23/2015 Washington Post article, "In the nation’s capital, a new business to regulate: D.C.’s personal trainers":
The article also discusses some of the controversy within the CrossFit community. (I don't do CrossFit, but this part might be interesting to my friends who do.)

From the 8/23/2015 Washington Post article, "In the nation’s capital, a new business to regulate: D.C.’s personal trainers":
The new regulations, being written by and for the nation’s capital city, will create a registry of all personal trainers in the District only. But they are expected to become a model that winners and losers in the fight believe will be replicated elsewhere.Personally, I find the idea of an agency deciding "who has the right to tell someone how to exercise" to be deeply disturbing.
The credit — or blame — for the newfound urgency can be traced in part to President Obama’s Affordable Care Act. A variety of workplace wellness programs and preventive health-care initiatives called for in the law could soon translate into rivers of billable hours for those with credentials to keep American waistlines in check.
And that means the race is on to be eligible for those credentials, which could eventually lead to the ability to bill insurance companies for services, much like such professionals as dieticians and physical therapists. With billions of dollars potentially at stake, lawyers and lobbyists are engaged in a no-holds-barred fight to shape the nation’s first-ever rules over who has the right to tell someone else how to exercise.
The article also discusses some of the controversy within the CrossFit community. (I don't do CrossFit, but this part might be interesting to my friends who do.)
Friday, August 21, 2015
Dinosaurs Are Dangerous!
Today's not-an-Onion story, "The day I removed a toy dinosaur from a woman's vagina".
There are very few jobs in which one gets paid to say things like, "I don’t advise inserting children’s toys during sexual activity, however if you do choose to masturbate with a toy dinosaur, I recommend buying your own, and perhaps putting it in a condom, or tying a leash to its foot."

There are very few jobs in which one gets paid to say things like, "I don’t advise inserting children’s toys during sexual activity, however if you do choose to masturbate with a toy dinosaur, I recommend buying your own, and perhaps putting it in a condom, or tying a leash to its foot."
Wednesday, August 19, 2015
"Never Events" and Unintended Consequences
Doctors (like all people) respond to incentives. Here's one "unintended consequence" of the policy of "never events", as explained by orthopedic surgeon Dr. Thomas Guastavina:
"The sad story of how “never events” prevent obese patients from getting new hips"

"The sad story of how “never events” prevent obese patients from getting new hips"
Monday, August 17, 2015
Uber For Health Care
WSJ: "Startups Vie to Build an Uber for Health Care".
There are some interesting business models in play:
It's also a win-win for participating doctors:

There are some interesting business models in play:
Heal is one of several startups putting a high-tech spin on old-fashioned house calls—or “in-person visits,” since they can take place anywhere. The services provide a range of nonemergency medical care—from giving flu shots to treating strep throats and stitching lacerations—much like a mobile urgent-care clinic.The article also notes that for some customers, it's cheaper to pay for this at-home service than to take time off from work to go to the doctor's office.
The companies use slightly different models. Pager, in New York City, dispatches doctors or nurse practitioners via Uber, for $200. Heal, in Los Angeles, San Francisco and Orange County, Calif., promises to “get a doctor to your sofa in under an hour” for $99. (A medical assistant goes along to do the driving and parking.)
RetraceHealth, in Minneapolis, has a nurse practitioner consult with patients via video (for $50), and only comes to their homes if hands-on care like a throat swab or blood draw is necessary (for $150)...
Most of the services don’t accept insurance, but they say patients can pay with health savings accounts or submit out-of-network claims.
It's also a win-win for participating doctors:
Such ventures are fueled by a confluence of trends, including growing interest in the so-called sharing economy, where technology connects providers with excess capacity and consumers who want on-demand services. Many doctors and nurses who work for hospitals are eager for extra work in their off-hours, the companies say. The services carry malpractice insurance, but say overall low overhead keeps prices down.I just hope the government doesn't impose onerous regulatory burdens on this growing sector.
And thanks to the boom in mobile-medical technology, providers can carry key equipment with them, from portable blood analyzers to hand-held ultrasounds.
Tuesday, August 11, 2015
Catron Takes Down Trump On Health Care
In his latest American Spectator piece, David Catron does a thorough take-down of Donald Trump on health care policy: "Trump Is No Friend of Free Market Health Care".
Here is the opening:
For more details, read the full text of "Trump Is No Friend of Free Market Health Care".
Here is the opening:
Most of Donald Trump’s public statements include the rote declaration that Obamacare is a disaster. This is true, of course, but it doesn’t tell us anything new. It’s only when he starts elaborating on his objections that one gets a sense of what he believes, and he doesn’t talk like a friend of the free market. During last week’s Republican debate, for example, he was asked about his past praise of single-payer health care and replied, “As far as single-payer, it works in Canada, works incredibly well in Scotland.” This answer was both antithetical to free-market thinking and profoundly ignorant...
For more details, read the full text of "Trump Is No Friend of Free Market Health Care".
Monday, August 10, 2015
Hsieh Forbes Column: Free Speech 1, FDA 0
My latest Forbes column is now out: "Free Speech 1, FDA 0".
I discuss a breaking update to my earlier Forbes piece on drug company Amarin's fight to engage in free speech in the form of off-label marketing of one of its products.
Basically, Amarin wanted to give truthful medical information to doctors which would allow them to more effectively use one of their drugs in a way that was legal, but not FDA-approved. The FDA forbade Amarin from engaging in such speech, and Amarin sued the FDA.
This past Friday, Amarin won an important legal victory in federal court. Judge Paul Engelmayer came down firmly on the side of free speech.
For more details see the full text of, "Free Speech 1, FDA 0".
(Earlier Forbes piece, "Drug Company Amarin Stands Up For Free Speech Against FDA", 5/8/2015.)
Update: Related commentary from Alex Tabarrok, "FDA Loses Another Free Speech Case"

I discuss a breaking update to my earlier Forbes piece on drug company Amarin's fight to engage in free speech in the form of off-label marketing of one of its products.
Basically, Amarin wanted to give truthful medical information to doctors which would allow them to more effectively use one of their drugs in a way that was legal, but not FDA-approved. The FDA forbade Amarin from engaging in such speech, and Amarin sued the FDA.
This past Friday, Amarin won an important legal victory in federal court. Judge Paul Engelmayer came down firmly on the side of free speech.
For more details see the full text of, "Free Speech 1, FDA 0".
(Earlier Forbes piece, "Drug Company Amarin Stands Up For Free Speech Against FDA", 5/8/2015.)
Update: Related commentary from Alex Tabarrok, "FDA Loses Another Free Speech Case"
Monday, August 3, 2015
UK Health Coverage
From EP Monthly:
"Man in Great Britain mugged, had his bicycle stolen, and had his leg broken in the process. He called emergency services, but was told that his injury 'wasn’t serious enough' to send an ambulance. Three police officers gave him a ride home where he had to book an Uber ride to get him to the hospital. Good thing he had medical 'insurance,' though."

"Man in Great Britain mugged, had his bicycle stolen, and had his leg broken in the process. He called emergency services, but was told that his injury 'wasn’t serious enough' to send an ambulance. Three police officers gave him a ride home where he had to book an Uber ride to get him to the hospital. Good thing he had medical 'insurance,' though."
Wednesday, July 29, 2015
Hsieh Forbes Column: Genuine Charity Requires Freedom
My latest Forbes column is now up: "Genuine Charity Requires Freedom".
I discuss the case of the amazingly generous man James Harrison, whose voluntary charity has helped save the lives of 2 million Australian babies. In Harrison's case, he literally gave of himself to help others in the form of over 1,100 voluntary blood donations.
I then discuss the nature of charity, why it requires freedom, and how compulsory "giving" destroy the morality of charity.
For more details, read the full text of "Genuine Charity Requires Freedom".

I discuss the case of the amazingly generous man James Harrison, whose voluntary charity has helped save the lives of 2 million Australian babies. In Harrison's case, he literally gave of himself to help others in the form of over 1,100 voluntary blood donations.
I then discuss the nature of charity, why it requires freedom, and how compulsory "giving" destroy the morality of charity.
For more details, read the full text of "Genuine Charity Requires Freedom".
Tuesday, July 28, 2015
Hsieh PJM Column: "In Praise Of The Market Economy"
PJ Media has posted my latest short column, "In Praise of the Market Economy".
One of my take-home points is that the prosperity created by the modern market economy creates both material and spiritual freedom unimaginable to our ancestors of 200 years ago.

One of my take-home points is that the prosperity created by the modern market economy creates both material and spiritual freedom unimaginable to our ancestors of 200 years ago.
Friday, July 24, 2015
Unintended Consequences Of Grading Doctors
Dr. Sandeep Jauhar has a nice piece in the 7/22/2015 New York Times, "Giving Doctors Grades".
He discusses some of the negative unintended consequences of "report cards" that supposedly rate a surgeon's quality based on patient mortality and complication outcome data. In essence, they discouraged surgeons from taking on the tougher cases and instead created a perverse incentive for them to "cherry pick" only the healthiest patients.
He cited experience from New York state, which has used such report cards since the 1990s:
He discusses some of the negative unintended consequences of "report cards" that supposedly rate a surgeon's quality based on patient mortality and complication outcome data. In essence, they discouraged surgeons from taking on the tougher cases and instead created a perverse incentive for them to "cherry pick" only the healthiest patients.
He cited experience from New York state, which has used such report cards since the 1990s:
They often penalized surgeons, like the senior surgeon at my hospital, who were aggressive about treating very sick patients and thus incurred higher mortality rates. When the statistics were publicized, some talented surgeons with higher-than-expected mortality statistics lost their operating privileges, while others, whose risk aversion had earned them lower-than-predicted rates, used the report cards to promote their services in advertisements.And:
This was an insult that the senior surgeon at my hospital could no longer countenance. “The so-called best surgeons are only doing the most straightforward cases,” he said disdainfully. Research since then has largely supported his claim...
It's not that quality metrics are completely useless. But they can be dangerously misleading. And they can create perverse incentives that harm both patients and physicians. (Via H.R.)Surgical report cards are a classic example of how a well-meaning program in medicine can have unintended consequences. Of course, formulas have been developed to try to adjust for the difficulty of surgical cases and level the playing field. For example, a patient undergoing coronary bypass surgery who has no other significant diseases has an average mortality risk of about 1 percent. If the patient also has severe kidney dysfunction and emphysema, the risk of death increases to 10 percent or more. However, many surgeons believe that such formulas still underestimate surgical risk and do not properly account for intangible factors, such as patient frailty.The best surgeons tend to operate at teaching hospitals, where the patients are the most challenging, but you wouldn’t know it from mortality statistics. It’s like high school students’ being penalized for taking Advanced Placement courses. College admissions officers are supposed to adjust grade point averages for difficulty of coursework, but as with surgical report cards, the formulas are far from perfect.The problem is compounded by the small number of operations — no more than 100 per year — that a typical cardiac surgeon performs. Basic statistics tell us that the “true” mortality rate of a surgeon is not what you measure after a small number of operations. The smaller the sample, the greater the deviation from the true average.
Wednesday, July 22, 2015
Dropout Doctors
An interesting new article discusses, "Dropout Docs: Bay Area Doctors Quit Medicine to Work for Digital Health Startups"
One quote from the article:

One quote from the article:
Tech culture is very appealing when juxtaposed against the hierarchy and myriad hoops to be jumped through in clinical medicine.Another quote:
Many of the dropout docs expressed a desire to improve the doctor-patient experience. In interviews with KQED, several said they spent very little time administering care during medical school, and they felt that patients were too often kept out of the loop.If young physicians find entrepreneurship more rewarding than clinical medicine, perhaps those who are setting the rules governing clinical medicine need to re-examine their policies. Until then, med school graduates should pursue whatever careers that they find the most professionally and personally satisfying.
A recent study found that doctors-in-training spend an average of just eight minutes with each patient. This is a drastic decrease from previous generations and is linked to more record-keeping requirements and restricted on-duty hours.
Thursday, July 16, 2015
VA Backlog
From the Huffington Post (7/13/2015): "Leaked Document: Nearly One-Third Of 847,000 Vets With Pending Applications For VA Health Care Already Died"
Tuesday, July 14, 2015
The Power Of "I Don't Know"
From John Tamny at Forbes: "'I Don't Know': The Ideal Libertarian And Conservative Response To Obamacare's Failings".
It's important to combat the notion of central planning with freedom, not merely an alternative version of central planning. By definition, freedom can yield new solutions not anticipated by anyone ahead of time.
It's important to combat the notion of central planning with freedom, not merely an alternative version of central planning. By definition, freedom can yield new solutions not anticipated by anyone ahead of time.
Tuesday, July 7, 2015
Hsieh Quoted on Guns And Public Health In US News & World Report
Today's US News & World Report had a nice piece on the debate over whether gun violence should be considered a "public health" issue, and they quoted me as explaining why it should not be:

But some medical providers say doctors should stay out of the debate. Dr. Paul Hsieh, co-founder of Freedom and Individual Rights in Medicine, says he views gun crime and violence as predominantly about criminal justice and individual rights.I thought they characterized my views fairly, and I was pleasantly surprised to see that they even turned the quote into one of the lead article graphics!
"I remain deeply skeptical of any attempts to frame important public policy debates as also 'public health' issues, especially when it concerns a long-running political controversy," says Hsieh, who writes on health care policy from a free-market perspective for Forbes.com. "Pretty much any public policy issue will ultimately have some sort of effects on the lives and well-being of Americans – but that doesn't mean they should all be considered topics of 'public health.'"
People are concerned that sharing information about gun ownership with doctors may not remain private, he wrote in a Forbes piece. "In short, I believe this undermines the critical doctor-patient trust necessary for the good practice of medicine," he says.
{kind=link}

Wednesday, July 1, 2015
Why CON Laws Need To Be Eliminated
"How State Certificate-of-Need (CON) Laws Affect Access to Health Care"
Monday, June 29, 2015
Hsieh Forbes Column: 3 Good Things In Health Care Innovation
My latest Forbes column is now up, "Three Good Things In Health Care Innovation".
I highlight some under-appreciated good developments in health care, centered around the theme that innovations in processes may be less flashy than innovations in technology — but can still save lives.
In particular, I discuss the following:
For more details on each, read the full text of "Three Good Things In Health Care Innovation".

I highlight some under-appreciated good developments in health care, centered around the theme that innovations in processes may be less flashy than innovations in technology — but can still save lives.
In particular, I discuss the following:
1) Improvements in cardiac careOur current system is very mixed, with both good and bad elements. Today, I wanted to focus on some of the good elements.
2) Improvements in matching kidney transplant donors with recipients
3) Protecting the freedom of direct pay doctors
For more details on each, read the full text of "Three Good Things In Health Care Innovation".
Friday, June 26, 2015
Cowen On King
Naturally, there has been an enormous amount of commentary on the SCOTUS ruling yesterday salvaging the ObamaCare subsidies.
The quote I liked the best comes from economist Tyler Cowen:

The quote I liked the best comes from economist Tyler Cowen:
I have not been a fan of Obamacare, which I consider to be a highly inefficient form of wealth insurance. Nonetheless, had this decision gone the other way at this point we would have ended up with something worse, or ended back at “Obamacare as know it,” but only after a lot of political stupidity and also painful media coverage. So on net I take this to be good news, although arguably it is bad news that it is good news.
Thursday, June 25, 2015
Bad Anesthesiologist Busted By Patient Recording
A patient planned to use his smartphone to record his post-colonoscopy home instructions. When he listend afterwards, he found that he inadvertently recorded the whole procedure, including while he was unconscious during sedation.
To his dismay, this included extremely unprofessional discussions:
On a related note, I do think that patients should consider recording their conversations with doctors in an open fashion, with mutual consent. I discuss this in my recent Forbes piece, "Why You Should Record Your Doctor Visits" (Forbes, 2/16/2015.)
(Pictured below, Dr. Tiffany Ingham, the anesthesiologist in question. Image from Washington Post article cited above.)

To his dismay, this included extremely unprofessional discussions:
But as soon as he pressed play on his way home, he was shocked out of his anesthesia-induced stupor: He found that he had recorded the entire examination and that the surgical team had mocked and insulted him as soon as he drifted off to sleep.The patient sued and was awarded total damages of $500,000. For more details read the full piece, "Anesthesiologist trashes sedated patient — and it ends up costing her" (Washington Post, 6/23/2015).
In addition to their vicious commentary, the doctors discussed avoiding the man after the colonoscopy, instructing an assistant to lie to him, and then placed a false diagnosis on his chart.
On a related note, I do think that patients should consider recording their conversations with doctors in an open fashion, with mutual consent. I discuss this in my recent Forbes piece, "Why You Should Record Your Doctor Visits" (Forbes, 2/16/2015.)
(Pictured below, Dr. Tiffany Ingham, the anesthesiologist in question. Image from Washington Post article cited above.)
Tuesday, June 23, 2015
Coverage Vs Care in California
Today's "coverage does not equal care" story, this time from California:
"Getting A Medi-Cal Card Doesn’t Always Guarantee Health Care" (Kaiser Health News, 6/23/2015)
(Unfortunately, the article promotes the idea that the problem can be solved by more regulatory intervention. I suspect that will only make things worse.)
"Getting A Medi-Cal Card Doesn’t Always Guarantee Health Care" (Kaiser Health News, 6/23/2015)
(Unfortunately, the article promotes the idea that the problem can be solved by more regulatory intervention. I suspect that will only make things worse.)
Wednesday, June 17, 2015
Summit At The Summit, July 20-26, 2015
The "Let My Doctor Practice" medical advocacy group will be hosting a conference July 20-26, 2015, here in Colorado.
It is entitled, "Summit at the Summit: Conference and Interactive Webcast A National Grand Rounds on the State of American Medicine".
They will have both a live in-person conference as well as a webcast, so you don't have to travel to Colorado to see some of the sessions.
I can't attend due to important personal obligations, but the lineup looks great!

It is entitled, "Summit at the Summit: Conference and Interactive Webcast A National Grand Rounds on the State of American Medicine".
They will have both a live in-person conference as well as a webcast, so you don't have to travel to Colorado to see some of the sessions.
I can't attend due to important personal obligations, but the lineup looks great!
Tuesday, June 9, 2015
Upcoming Talk By Paul Hsieh: "How Do You Know If Your Doctor Is Any Good?"
Save the date -- June 22, 2015!
I'm pleased to announce that I'll be giving a dinner talk at Liberty On The Rocks - Flatirons on 6/22/2015. More details will be forthcoming at their website and their Facebook page, but here's the basic info.
Title: "How Do You Know If Your Doctor Is Any Good?" by Paul Hsieh, MD
Description:
I'm pleased to announce that I'll be giving a dinner talk at Liberty On The Rocks - Flatirons on 6/22/2015. More details will be forthcoming at their website and their Facebook page, but here's the basic info.
Title: "How Do You Know If Your Doctor Is Any Good?" by Paul Hsieh, MD
Description:
How do you know if your doctor is giving you the best medical advice
possible? Or offering the right care for your condition? Most patients
lack the professional training to judge a doctor's qualifications, so
they must rely on various proxy measures, such as referrals from other
doctors, recommendations from friends, government ratings, and online
reviews. We'll discuss some of the strengths and weaknesses of these
measures as well as practical steps patients can take to ensure they're
receiving the best care possible.
Speaker bio:

Paul Hsieh, MD, is a physician in private practice in the south Denver metro area. He received his MD from University of Michigan, and completed residency training at Washington University School of Medicine with additional fellowship training at the Cedars-Sinai Medical Center in Los Angeles. He writes extensively about health care policy from a free market perspective for Forbes and PJ Media.
Spoiler: You probably don't want this guy operating on you!

Speaker bio:

Paul Hsieh, MD, is a physician in private practice in the south Denver metro area. He received his MD from University of Michigan, and completed residency training at Washington University School of Medicine with additional fellowship training at the Cedars-Sinai Medical Center in Los Angeles. He writes extensively about health care policy from a free market perspective for Forbes and PJ Media.
Spoiler: You probably don't want this guy operating on you!

Monday, June 8, 2015
Doctors Afraid To Criticize ObamaCare?
This IBD editorial discusses how, "Doctors' Criticism Of ObamaCare Silenced By ACA Bureaucrats".
I've personally not felt any professional pressure to refrain from expressing political opinions online. But I do know some doctors who have. Which is why I gladly support those physicians who still have the guts and integrity to speak out on this issue.
I've personally not felt any professional pressure to refrain from expressing political opinions online. But I do know some doctors who have. Which is why I gladly support those physicians who still have the guts and integrity to speak out on this issue.
Thursday, June 4, 2015
More Health IT Costs
Politico reports: "Health care spending billions to protect the records it spent billions to install".
From the article:
From the article:
The hacking of the health records of as many as 1 in 3 Americans has awoken the health care industry to an unpleasant reality: After spending billions to install computerized documents in hospitals and networks, it now must spend billions more to make them secure...Yet another "unintended consequence" of government-mandated electronic health records.
Wednesday, June 3, 2015
Malpractice and Communications
From the New York Times: "To Be Sued Less, Doctors Should Consider Talking to Patients More".
Monday, June 1, 2015
Hsieh Forbes Column: Would You Trust A Computer To Knock You Out?
I posted a quick weekend piece at Forbes, "Would You Trust A Computer To Knock You Out?"
This is loosely based on a talk I just gave at ATLOSCon 2015, "I, For One, Welcome Our New Robotic Overlords".
I discuss the rise of "smart" systems to augment (and potentially replace) human physicians. And why I welcome them.
And thanks to Hanah Volokh for letting me quote her!

This is loosely based on a talk I just gave at ATLOSCon 2015, "I, For One, Welcome Our New Robotic Overlords".
I discuss the rise of "smart" systems to augment (and potentially replace) human physicians. And why I welcome them.
And thanks to Hanah Volokh for letting me quote her!

Wednesday, May 27, 2015
Maine Doctors Choosing Direct Pay Model
From Maine Public Radio: "Awash in Paperwork, Maine Doctors Abandon Conventional Treatment Model".
More real-world experience shows how direct-pay medicine benefits both patients and physicians alike. From the piece:
In summary:

More real-world experience shows how direct-pay medicine benefits both patients and physicians alike. From the piece:
[Family physician Dr. Catherine] Krouse says the way health care has evolved, patients often come second to the other demands on doctors: Filling out reimbursement forms. Calling insurance companies to battle for claims. Reviewing and signing off on stacks of patient paperwork.
"You just end up getting drained and drained and drained," Krouse says. "And then when your cup is completely empty, then you just get guarded and angry. And then you put up walls, and that really creates barriers."
So Krouse decided to set up a direct primary care practice. Earlier this month she opened Lotus Family Practice in Falmouth. She doesn't accept insurance. Instead, she charges patients a monthly membership fee. "So it's very direct. It's just patients and doctors. There's no one else in between."
Membership is $60 a month for adults, $20 for kids. It covers an unlimited number of visits, which last about 45 minutes. Patients can also call or text Krouse any time they want. She also provides generic drugs at wholesale cost. Those savings alone, she says, can cover the cost of membership. "Pennies. They cost pennies."The article goes into more detail on how this helps physicians spend more time with patients and get to the root of their health problems. Plus patients need fewer referrals to specialists.
In summary:
The direct primary care model, [Krouse] says, allows her to move beyond just treating illness to focusing on health, well being, and the individual patient. And that's the kind of doctor that Krouse has always wanted to be.(Article link via Dr. Megan Edison and Dr. Matthew Bowdish.)
Wednesday, May 13, 2015
Unethical Doctors
There are some jaw-dropping stories here: "Doctors of Reddit, what is the most unethical thing you have done or you have heard of a fellow doctor doing involving a patient?"
For those following health care policy, this anecdote is relevant:
For those following health care policy, this anecdote is relevant:
I briefly worked at the front desk clerk for an ER at a local hospital. The rule was the anyone that came in complaining of chest pains had to be back and on a machine within 10 minutes of arrival. Once I entered their name into the system a clock started. So I was told not to enter their name until they had already been taken back to essentially make our numbers look better and make it appear as though they were receiving care within the prescribed 10 minutes.(Via White Coat blog.)
Edit: People complaining of chest pains were typically brought back quickly, just not always within the 10 minute guideline, although generally faster than anyone else. This mostly seemed to be just about producing better stats. Although keeping it off the system gave them the ability to delay.
"There are three kinda lies in the world; lies, damned lies, and statistics."
Friday, May 8, 2015
Hsieh Forbes Column: FDA Vs. Free Speech
My latest Forbes column is now up: "Drug Company Amarin Stands Up For Free Speech Against FDA".
Here is the opening:
But both doctors and patients benefit when drug companies are allowed to publish truthful information.
Bonus infographic on the onerous FDA approval process!

Here is the opening:
Even as Americans heatedly argue the issue of free speech with respect to cartoon criticisms of Islam, the small drug company Amarin is striking a quieter blow for its free speech rights against the Food and Drug Adminstration (FDA).Of course, drug companies should not be allowed to disseminate false or misleading information about their products. That can and should be punished as fraud.
The key issue is whether drug companies can tell doctors truthful information about their products that pertains to “off-label” uses (i.e., for applications not already explicitly approved by the FDA.)
But both doctors and patients benefit when drug companies are allowed to publish truthful information.
Bonus infographic on the onerous FDA approval process!
Friday, May 1, 2015
Wednesday, April 29, 2015
Cleveland Clinic Empathy Video
This is change of pace from the health policy posting.
But I wanted to share this moving short video from the Cleveland Clinic on the hundreds of behind-the-scenes stories every day in the hospital. (I recently saw it a medical conference I attended earlier this month.)
Thank you.
But I wanted to share this moving short video from the Cleveland Clinic on the hundreds of behind-the-scenes stories every day in the hospital. (I recently saw it a medical conference I attended earlier this month.)
Thank you.
Monday, April 27, 2015
Hsieh Forbes Column: Perverse Incentives and VA Health Scandals
My latest Forbes column is now up: "Perverse Incentives and VA Health Scandals".
I discuss the perverse incentives underlying the numerous VA health scandal. Too many on the political Left (such as New York Times columnist Paul Krugman) are quick to condemn perverse incentives in the private health system, while failing to mention similar (or worse) perverse incentives in government-run health systems.
Incentives matter.

I discuss the perverse incentives underlying the numerous VA health scandal. Too many on the political Left (such as New York Times columnist Paul Krugman) are quick to condemn perverse incentives in the private health system, while failing to mention similar (or worse) perverse incentives in government-run health systems.
Incentives matter.
Tuesday, April 14, 2015
Doc Fix Critiques
Three recent negative critiques of the Medicare "Doc Fix":
"House 'Doc Fix' Bill Makes Things Worse, Medicare Analysis Finds" (Chris Jacobs, Wall Street Journal)
"Medicare Doc Fix Bill Is IPAB-Lite" (David Hogberg, Daily Caller)
"Medicare fix needs fixing" (Theodore Marmor, Philadelphia Inquirer)
In particular, the Hogberg piece notes the perverse incentives that will pressure doctors skimp on care to patients as part of cost containment. But all three are worth reading.

"House 'Doc Fix' Bill Makes Things Worse, Medicare Analysis Finds" (Chris Jacobs, Wall Street Journal)
"Medicare Doc Fix Bill Is IPAB-Lite" (David Hogberg, Daily Caller)
"Medicare fix needs fixing" (Theodore Marmor, Philadelphia Inquirer)
In particular, the Hogberg piece notes the perverse incentives that will pressure doctors skimp on care to patients as part of cost containment. But all three are worth reading.
Monday, April 13, 2015
Perry: Lessons From Cosmetic Surgery Markets
Economist Mark Perry has a written a nice review, "What economic lessons about health care can we learn from the market for cosmetic procedures?"
In general, these services are not covered by insurance but rather paid for by the consumers themselves. Hence, consumers have a keen interest in finding the best value for their medical dollar.
As a result, prices have essentially stayed stable (or decreased significantly) after adjusting for inflation. In some case, the prices have gone down in nominal dollars as well!
As Perry notes:
Proper treatment of a problem requires a proper diagnosis, in public policy as well as in medicine. Perry's work is an important pointer in the right direction.

In general, these services are not covered by insurance but rather paid for by the consumers themselves. Hence, consumers have a keen interest in finding the best value for their medical dollar.
As a result, prices have essentially stayed stable (or decreased significantly) after adjusting for inflation. In some case, the prices have gone down in nominal dollars as well!
As Perry notes:
Most importantly, none of the ten cosmetic procedures in the table above have increased in price by anywhere close to the 88.5% increase in medical care services since 1998. [Emphasis his.]Perry summarizes:
The competitive market for cosmetic procedures operates differently than the traditional market for health care in important and significant ways. Cosmetic procedures, unlike most medical services, are not usually covered by insurance. Patients paying out-of-pocket for cosmetic procedures are cost-conscious, and have strong incentives to shop around and compare prices at the dozens of competing providers in any large city.In other words, the problem we've seen of skyrocketing prices in the traditional medical market can't be blamed on "fee for service". Rather, the issue is the 3rd-party payor system, a point also made by others such as Dr. Richard Amerling in his recent Wall Street Journal piece.
Because of that market competition, the prices of almost all cosmetic procedures have fallen in real terms since 1998, and some non-surgical procedures have even fallen in nominal dollars before adjusting for price changes. In all cases, cosmetic procedures have increased in price by less than the 88.5% increase in the price of medical care services between 1998 and 2014.
Proper treatment of a problem requires a proper diagnosis, in public policy as well as in medicine. Perry's work is an important pointer in the right direction.
Subscribe to:
Posts (Atom)