My latest Forbes piece is now out, "No, The Government Should Not Provide Health Insurance For All Americans".
I discuss a proposal from conservative health policy analyst James Capretta in which he argues, "The GOP Should Provide Health Insurance for All Americans". And I propose some alternative free-market approaches that we can start implementing in 2017.
For more details, see the full text of "No, The Government Should Not Provide Health Insurance For All Americans".
And Happy New Year to all our supporters and subscribers!
The blog of Freedom and Individual Rights in Medicine (FIRM)
Thursday, December 29, 2016
Monday, November 28, 2016
Hsieh Forbes Column: UK Vs US Aortic Aneurysm Deaths
My latest Forbes pieces is now out: "Patients With Aortic Aneurysms More Likely To Die In The UK Than The US".
I discuss a recent New England Journal of Medicine study which showed that if you have an abdominal aortic aneurysm (aka "AAA") in the US vs the UK, the UK patients have to wait longer for surgery, and the aneurysms don't get repaired until they are larger (and more at risk of rupture.)
The researchers conclude: "Rates of aneurysm rupture and aneurysm-related death were significantly higher in England than in the United States".
I also cover three natural follow-up questions:
1) Were US surgeons jeopardizing their patients by operating more aggressively than UK surgeons?
2) Did the UK nationalized health system contribute to the lower rates of appropriate surgery in the UK?
3) Will US government policies incentivize American surgeons towards more — or less — appropriate treatments?
For more details, read the full text of "Patients With Aortic Aneurysms More Likely To Die In The UK Than The US".

I discuss a recent New England Journal of Medicine study which showed that if you have an abdominal aortic aneurysm (aka "AAA") in the US vs the UK, the UK patients have to wait longer for surgery, and the aneurysms don't get repaired until they are larger (and more at risk of rupture.)
The researchers conclude: "Rates of aneurysm rupture and aneurysm-related death were significantly higher in England than in the United States".
I also cover three natural follow-up questions:
1) Were US surgeons jeopardizing their patients by operating more aggressively than UK surgeons?
2) Did the UK nationalized health system contribute to the lower rates of appropriate surgery in the UK?
3) Will US government policies incentivize American surgeons towards more — or less — appropriate treatments?
For more details, read the full text of "Patients With Aortic Aneurysms More Likely To Die In The UK Than The US".
Tuesday, October 25, 2016
Hsieh Forbes Column: How Your Doctor's Politics Affects Your Health Care
My latest Forbes piece is now out, "How Your Doctor's Politics Affects Your Health Care -- And What You Can Do About It".
I discuss the latest research indicating the doctors' own personal political biases can affect the advice they give patients in three areas -- abortion, gun ownership, and marijuana use. And strategies that patients and doctors can adopt to minimize inappropriate physician bias in the exam room.

I discuss the latest research indicating the doctors' own personal political biases can affect the advice they give patients in three areas -- abortion, gun ownership, and marijuana use. And strategies that patients and doctors can adopt to minimize inappropriate physician bias in the exam room.
Friday, September 16, 2016
Hsieh Forbes Column: No, There's No 'Smoking Gun' in Clinton's Doctor Letter
I have a new short Forbes piece out now, discussing a couple of issues related to Hillary Clinton's health: "No, There's No 'Smoking Gun' in Clinton's Doctor Letter".
tldr; Clinton's opponents should concentrate on her bad public policy positions, not her medical record.
tldr; Clinton's opponents should concentrate on her bad public policy positions, not her medical record.
Monday, August 29, 2016
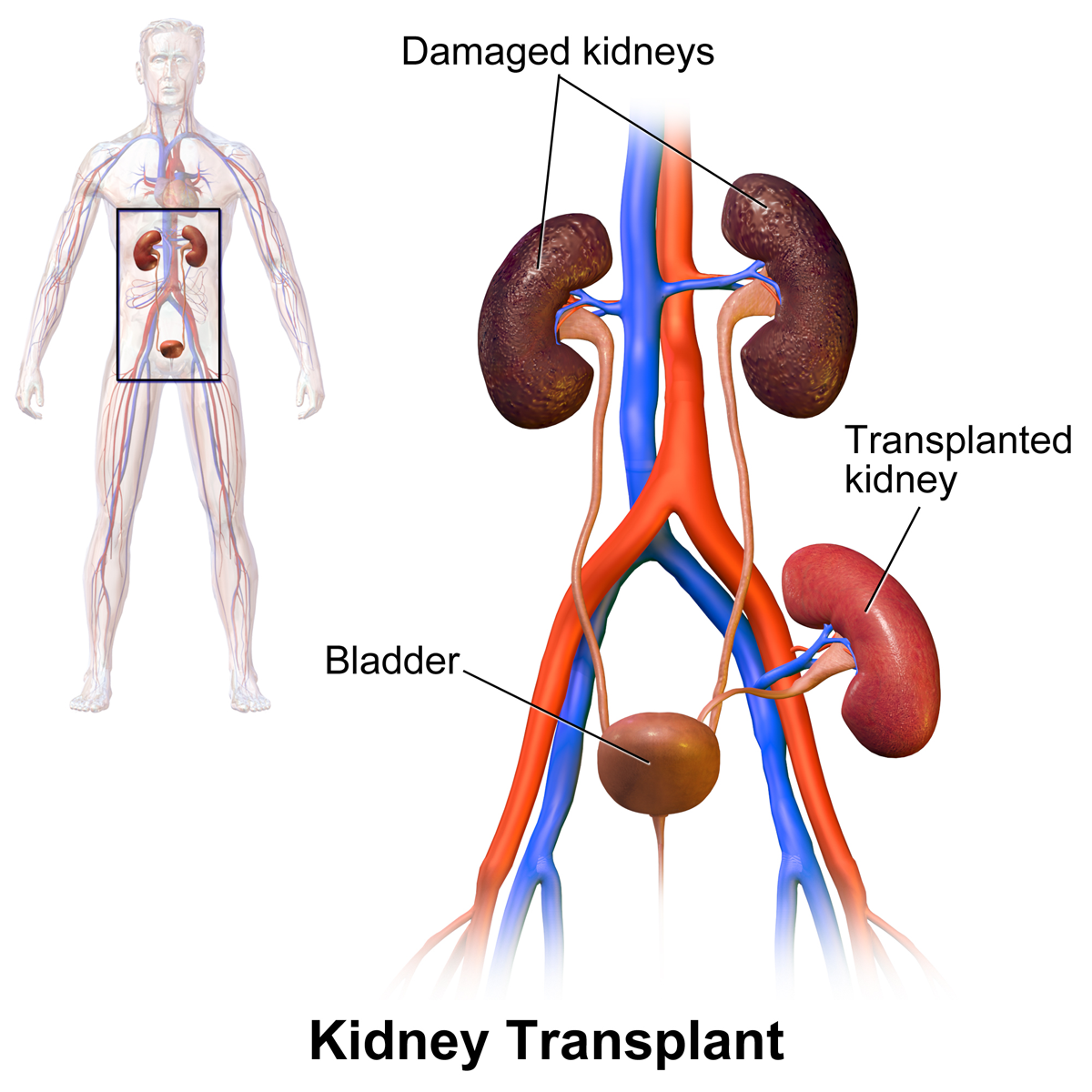
Hsieh Forbes Column: How Government Quality Guidelines Hurt Transplant Patients
My latest Forbes piece is now up: "How Government Quality Guidelines Hurt Transplant Patients".
I discuss how federal government "quality guidelines" created perverse incentives to deny medical care to the sickest patients.
In particular, many transplant centers started dropping the sickest patients from their transplant waiting lists in order to keep their success rates up. Plus many hospitals rejected less-than-perfect organs out of fear of harming their federal government score cards.
As transplant surgeon Dr. Adel Bozorgzadeh said:
For more details, read the full text of "How Government Quality Guidelines Hurt Transplant Patients".
(Related piece: "Doctor ‘Report Cards’ May Be Hazardous To Your Health.")
I discuss how federal government "quality guidelines" created perverse incentives to deny medical care to the sickest patients.
In particular, many transplant centers started dropping the sickest patients from their transplant waiting lists in order to keep their success rates up. Plus many hospitals rejected less-than-perfect organs out of fear of harming their federal government score cards.
As transplant surgeon Dr. Adel Bozorgzadeh said:
“If you have young guy who has a 100 percent chance of dying, but only a 30 percent chance of dying with a transplant, you would say, ‘What the hell, give the guy a chance,’” even if the operation might be risky, he said. “But if I make an argument like that, I will be under pressure from all these other stakeholders who would penalize me.”The federal guidelines created a conflict of interest for hospitals, caught between their government paymasters and the patients they were supposed to care for.
For more details, read the full text of "How Government Quality Guidelines Hurt Transplant Patients".
(Related piece: "Doctor ‘Report Cards’ May Be Hazardous To Your Health.")
Tuesday, August 2, 2016
FIRM Website Problems Fixed
My deepest apologies for the recent downtime of the FIRM website. And many thanks to my ex-wife Diana Brickell for fixing the DNS issues! I should be back in action soon.
Friday, June 24, 2016

Wednesday, June 22, 2016
Hsieh Forbes Column: Why I Don't Trust Government-Backed 'Gun Violence' Research
My latest Forbes piece is now out: "Why I Don't Trust Government-Backed 'Gun Violence' Research".
I discuss the anti-gun bias at the federal government Centers For Disease Control (CDC) and why we should be suspicious of calls for more CDC-backed research into "gun violence".

I discuss the anti-gun bias at the federal government Centers For Disease Control (CDC) and why we should be suspicious of calls for more CDC-backed research into "gun violence".
Wednesday, June 15, 2016
When Everything Is "Critical", Then Nothing Is
Another consequence of poorly designed electronic medical records (EMRs) is "alert fatigue":

Electronic health records increasingly include automated alert systems pegged to patients’ health information. One alert might signal that a drug being prescribed could interact badly with other medications. Another might advise the pharmacist about a patient’s drug allergy. But they could also simply note each time that a patient is prescribed painkillers — useful to detect addiction but irrelevant if, say, someone had a major surgery and is expected to need such meds. Or they may highlight a potential health consequence relevant to an elderly woman, although the patient at hand is a 20-something man.This can have real-life consequences:
The number of these pop-up messages has become unmanageable, doctors and IT experts say, reflecting what many experts call excessive caution, and now they are overwhelming practitioners.
Clinicians ignore safety notifications between 49 percent and 96 percent of the time, said Shobha Phansalkar, an assistant professor of medicine at Harvard Medical School.
“When providers are bombarded with warnings, they will predictably miss important things,” said David Bates, senior vice president at Brigham and Women’s Hospital in Boston.
In one instance at Children’s [Hospital of Philadelphia], doctors ignored relevant information about how a patient might respond to a drug, Shelov said, because it appeared alongside heaps of other superfluous notifications — warnings, for instance, about drugs that posed minimal risk of interfering with each other. Consequently, the patient received medication that induced a potentially lethal reaction.When everything is "critical", then nothing is.
The hospital caught the mistake in time, but the incident spurred a series of changes. A team of pharmacists, doctors and other clinicians have sorted through what triggered alerts in their system, turning off the ones they decided weren’t actually relevant or necessary. That has helped. But it’s still an ongoing battle, Shelov said. “It’s a little bit of trying to turn off the firehose.”
Monday, June 13, 2016
Doctors And Handwashing
"What is doctors' compliance rate for hand hygiene procedures?"
As Tyler Cowen says:

As Tyler Cowen says:
According to a new study, when they know they are being watched it is 57 percent.
When they don’t know they are being watched, it is 22 percent.
What I find shocking is not the difference, which fits readily into the economic way of thinking. It is that direct observation of doctors still does not get the rate above 57 percent.
Tuesday, May 31, 2016
Hsieh Forbes Column: Three Tales of Health, Technology, and Freedom
My latest Forbes piece is now out: "Three Tales of Health, Technology, and Freedom".
I highlight recent stories on the "artificial pancreas", research into Chronic Fatigue Syndrome, and patients ordering their own blood tests.
When people pursue important health goals, often the government helps best by getting out of the way.
I highlight recent stories on the "artificial pancreas", research into Chronic Fatigue Syndrome, and patients ordering their own blood tests.
When people pursue important health goals, often the government helps best by getting out of the way.
Friday, May 13, 2016
Dad Of The Year
From the Wall Street Journal, "Tech-Savvy Families Use Home-Built Diabetes Device":
Third-grader Andrew Calabrese carries his backpack everywhere he goes at his San Diego-area school. His backpack isn’t just filled with books, it is carrying his robotic pancreas.Unfortunately, the FDA isn't particularly supportive of such grass-roots endeavors.
The device, long considered the Holy Grail of Type 1 diabetes technology, wasn’t constructed by a medical-device company. It hasn’t been approved by regulators.
It was put together by his father...
Friday, April 29, 2016
Hsieh Forbes Column: Protect Physician Free Speech In The Office Visit
My latest Forbes column is now out: "Protect Physician Free Speech In The Office Visit".
Should politicians dictate what physicians must (or must not) say to patients when it comes to contentious political issues like abortion or gun ownership? I say, "no".

Should politicians dictate what physicians must (or must not) say to patients when it comes to contentious political issues like abortion or gun ownership? I say, "no".
Monday, April 25, 2016
Wednesday, April 13, 2016
Transplant Woes
An unfortunate story: "The Search For A 'Perfect' Organ Cost My Wife Her Life". (Via @motivepwr.)
Monday, April 11, 2016
Human Stories Vs. Electronic Medical Records
Dr. Susan Koven describes how, "As hospitals go digital, human stories get left behind".
Dr. Koven described an encounter with a patient, with enormously rich detail. But when she had to record the information in the electronic medical records, the system hampered her ability to tie key connections together:

Dr. Koven described an encounter with a patient, with enormously rich detail. But when she had to record the information in the electronic medical records, the system hampered her ability to tie key connections together:
My warm feelings vanished as I sat down to document the visit. While I’ve used an electronic medical record for several years, Epic, the system my hospital recently adopted, makes recording stories such as the one my patient shared especially difficult. Her grief and her fatigue, which are inseparable in reality, Epic treats as different problems. That she lives alone and there’s conflict in her extended family, which are also inextricable from her symptoms, must be filed under a tab marked “Social Documentation.”The electronic records may make life easier for the hospital billing department. And they may make life easier for researchers trying to do population-based studies. But if it hampers the primary care physician's ability to actually care for the patient, we have a problem.
Epic features lists of diagnoses and template-generated descriptions of symptoms and physical examination findings. But it provides little sense of how one event led to the next, how one symptom relates to another, the emotional context in which the symptoms or events occurred, or the thought process of the physician trying to pull together individual strands of data into a coherent narrative. Epic is not well-suited to communicating a patient’s complex experience or a physician’s interpretation of that experience as it evolves over time, which is to say: Epic is not built to tell a story...
The risk of this format, as physician and medical informatics expert Dr. Robert Wachter points out in a blog post, is that we may forget that “patients are more than the sum of their problems.”
A medical record that abandons narrative in favor of a list does more than dehumanize our patients. It also hampers a clinician’s diagnostic abilities. Take a patient I saw recently, a middle-aged woman with palpitations. She was perimenopausal, stressed out at work, having trouble sleeping, drinking lots of coffee to stay awake during the day, and had a family history of heart disease. Any one of those issues might explain her palpitations, but more likely some combination of interrelated factors was causing them. Sorting out the story is crucial to deciding which tests to order and what treatment to recommend.
Friday, April 8, 2016
Patient Secretly Records Surgery And Hears Disturbing Conversations
From the 4/7/2016 Washington Post: "Patient secretly recorded doctors as they operated on her. Should she be so distressed by what she heard?"
Although I don't do surgery, I do sometimes perform invasive procedures on unconscious or sedated patients. I always speak as if the patient were fully awake and able to understand me.
One can debate the ethics of recording one's doctor when they aren't aware of it. I do fully support recording important doctor visits with the consent of both parties, as I discussed last year in, "Why You Should Record Your Doctor Visits".
Although I don't do surgery, I do sometimes perform invasive procedures on unconscious or sedated patients. I always speak as if the patient were fully awake and able to understand me.
One can debate the ethics of recording one's doctor when they aren't aware of it. I do fully support recording important doctor visits with the consent of both parties, as I discussed last year in, "Why You Should Record Your Doctor Visits".
Thursday, April 7, 2016
Assisted Suicide in California
News update: "Doctor-assisted dying will be legal in California from June 9th".
I recognize this is a controversial topic amongst many physicians. However, I support the basic idea in the interests of patient autonomy.
My own thoughts on this topic can be found in this January 2015 piece, "Does Your Right To Life Include The Right To Die?"
I recognize this is a controversial topic amongst many physicians. However, I support the basic idea in the interests of patient autonomy.
My own thoughts on this topic can be found in this January 2015 piece, "Does Your Right To Life Include The Right To Die?"
Thursday, March 31, 2016
Hsieh Forbes Column on The Great Canadian Sperm Crisis
My latest Forbes piece is now up: "The Market Solution To The Great Canadian Sperm Crisis".
A couple of facts:
* There is an enormous shortage of donated sperm in Canada, such that infertile couples have to rely on (gasp) imported sperm from the US.
* The Canadian government outlaws paying Canadian sperm donors for their product.
Hmm.... Could there possibly be any connection between these two facts?
For more details, read the full text of "The Market Solution To The Great Canadian Sperm Crisis".

A couple of facts:
* There is an enormous shortage of donated sperm in Canada, such that infertile couples have to rely on (gasp) imported sperm from the US.
* The Canadian government outlaws paying Canadian sperm donors for their product.
Hmm.... Could there possibly be any connection between these two facts?
For more details, read the full text of "The Market Solution To The Great Canadian Sperm Crisis".
Tuesday, March 15, 2016
Catron Critiques Trump
David Catron of The American Spectator has a pretty harsh critique of Donald Trump's health care plan from the conservative perspective in his 3/14/2016 piece, "Trumpcare: A Hazy Plan From a Lazy Man".
From the opening of Catron's piece:

From the opening of Catron's piece:
[T]ake a minute to peruse the health care proposal he has finally cobbled together and posted on his campaign website. And, rest assured, it won’t take more than a minute to read. Trump’s “plan” consists of seven random nostrums that appear to have been hastily cribbed from conservative and libertarian websites by his various flunkies. And it confirms yet again that neither “the Donald” nor his yes men are willing to do their homework...(Catron also offers some broader commentary on Trump's campaign and isn't impressed.)
Thursday, March 10, 2016
Small Free Speech Victory
The 3/8/2016 New York Times reports, "FDA Deal Allows Amarin to Promote Drug for Off-Label Use".
This is a small but potentially important victory for drug company free speech rights. As the articles notes:
And if any companies would like to further pursue this kind of free speech fight, they should contact attorney Jim Manley of the Goldwater Institute. Manley and the Goldwater Institute have urged policy changes in this area and are exploring litigation.
(Related story from last year: "Free Speech 1, FDA 0".)
This is a small but potentially important victory for drug company free speech rights. As the articles notes:
The agreement settles a legal case between the agency and the company, Amarin, a small drug maker that sued the F.D.A. last year for the right to promote its only product, Vascepa, to a broader range of patients. In August, a federal district judge in Manhattan ruled that the F.D.A. could not prohibit Amarin from using truthful information to promote its drug, even for unapproved uses, because doing so would violate the company’s right to free speech.The final settlement is still subject to approval by the court.The agency on Tuesday downplayed the implications of the deal. In a statement, it said that the settlement applied only to the Amarin case and that its position on whether companies have a constitutional right to provide truthful information about off-label uses had not changed.But some legal and drug-safety experts said the settlement could encourage other companies to seek similar arrangements and, ultimately, have profound implications for how drug makers sell their products...
Clearly, the FDA wishes to keep the scope of this as narrow as possible. On the other hand, many free speech advocates would like to see this principle applied more broadly.
And if any companies would like to further pursue this kind of free speech fight, they should contact attorney Jim Manley of the Goldwater Institute. Manley and the Goldwater Institute have urged policy changes in this area and are exploring litigation.
(Related story from last year: "Free Speech 1, FDA 0".)
Wednesday, March 2, 2016
Patient Safety and Electronic Medical Records
A good report from Kaiser Health News on what doctors in the trenches deal with regularly: "EHRs In The ER: As Doctors Adapt, Concerns Emerge About Medical Errors".
Here's the introduction:
Imagine how user friendly your smart phones would be, if you had to buy one (rather than choosing whether or not to get one.)
Unfortunately, patients will pay the price:
Most doctors try their best take good care of their patients. It's unfortunate when government technology mandates makes that job that harder, not easier.

Here's the introduction:
The mouse slips, and the emergency room doctor clicks on the wrong number, ordering a medication dosage that’s far too large. Elsewhere, in another ER’s electronic health record, a patient’s name isn’t clearly displayed, so the nurse misses it and enters symptoms in the wrong person’s file.In other words, EHRs were rammed down the throats of doctors and hospitals, rather than being allowed to be integrated organically according to the best judgments of the end users.
These are easy mistakes to make. As ER doctors and nurses grapple with the transition to digitalized record systems, they seem to happen more frequently.
“There are new categories of patient safety errors” in emergency rooms that didn’t exist before the push to use electronic record systems, said Raj Ratwani, who researches health care safety and is the scientific director for MedStar Health’s National Center for Human Factors in Healthcare in Washington, D.C.
Spurred by the 2009 stimulus package and the 2010 health reform law, the federal government has offered hospitals financial incentives to adopt electronic health records that, among other things, will add efficiency and reduce errors by linking physicians’ patient records, and coordinating and tracking how care is delivered across the health system. Hospitals that don’t meet those standards are hit with penalties...
Imagine how user friendly your smart phones would be, if you had to buy one (rather than choosing whether or not to get one.)
Unfortunately, patients will pay the price:
The ER’s culture and pace, for instance, can amplify the risks of human error that stem from an already less user-friendly system. Think of the emergency physician who, reaching the end of a hectic 12-hour shift, looks for the record of a patient he just examined. He types in the man’s last name, clicks and writes medical instructions — not realizing that he’d accidentally pulled up the file of another patient with the same last name and similar age, who was admitted five minutes before.For now, this means patients will have to be extra-diligent in confirming that the data in their health records is accurate. And that any prescriptions or treatments they receive actually make sense.
While misidentifying patients in this way was hardly an issue before EHRs, it’s “becoming quite prevalent,” in this more digital era, Ratwani said.
Most doctors try their best take good care of their patients. It's unfortunate when government technology mandates makes that job that harder, not easier.
Monday, February 29, 2016
Open Your Heart
Great talk by Dr. Jordan Winkler: "10 Easy Steps to Open Your Heart".
Funny and informative. Really. I'm really glad I live at time this is possible. Contains slightly NSFW language. (Via B.E.)
Funny and informative. Really. I'm really glad I live at time this is possible. Contains slightly NSFW language. (Via B.E.)
Monday, February 22, 2016
Cut Health Costs By Paying Cash
The Wall Street Journal explains, "How to Cut Your Health-Care Bill: Pay Cash".
Not long ago, hospitals routinely charged uninsured patients their highest rates, far more than insured patients paid for the same services. Now, in the Alice-in-Wonderland world of health-care prices, the opposite is often true: Patients who pay up front in cash often get better deals than their insurance plans have negotiated for them.
That is partly due to new state and federal rules aimed at protecting uninsured patients from price gouging. (Under the Affordable Care Act, for example, tax-exempt hospitals can’t charge financially strapped patients much more than Medicare pays.) Many hospitals also offer discounts if patients pay in cash on the day of service, because it saves administrative work and collection hassles. Cash prices are officially aimed at the uninsured, but people with coverage aren’t legally required to use it.
Friday, February 19, 2016
Update on Edison Vs. MOC
Dr. Megan Edison gives an important update on the MOC controversy, including practical steps physicians can take to defend their autonomy.
Thursday, February 18, 2016
Hsieh Forbes Post: Liberals Against Sanders On Health Economics
I have another short post in today's Forbes: "Liberals Against Sanders On Health Economics".
Many on the political Left are speaking out against Bernie Sanders' economic and health proposals. Their objections lie primarily in the realm of economics (rather than deeper issues of the proper scope of government). But nonetheless, the pushback Sanders is getting from fellow "progressives" has surprised me.
When you've lost Paul Krugman...
Many on the political Left are speaking out against Bernie Sanders' economic and health proposals. Their objections lie primarily in the realm of economics (rather than deeper issues of the proper scope of government). But nonetheless, the pushback Sanders is getting from fellow "progressives" has surprised me.
When you've lost Paul Krugman...
Wednesday, February 17, 2016
Hsieh Forbes Column: Americans Love This Deadly Technology
My latest Forbes piece is now out: "Americans Love This Deadly Technology".
The theme: Americans are willing to accept 32,000 deaths per year as the price of freedom.
The theme: Americans are willing to accept 32,000 deaths per year as the price of freedom.
Friday, February 5, 2016
Pregnancy Warnings In US, Australia, And France
Here's a helpful chart in case you are pregnant.
(This was likely in response to the latest paternalisic federal government recommendations as reported in USA Today, "CDC: Young women should avoid alcohol unless using birth control".)

(This was likely in response to the latest paternalisic federal government recommendations as reported in USA Today, "CDC: Young women should avoid alcohol unless using birth control".)

Tuesday, February 2, 2016
Armstrong On Insurance Vs. Care
Dr. Richard Armstrong of the Docs4PatientCare Foundation has another nice column out, "Why Health Insurance doesn't equal Health Care".
Armstrong's basic thesis is simple:
(Read the full text of, "Why Health Insurance doesn't equal Health Care".)
Armstrong's basic thesis is simple:
Health insurance as commonly “understood” is not true insurance. This is one of the significant causes of our current national misunderstanding of health care financing which underlines the importance of these educational efforts.But the details are important. He traces the transformation of insurance from simple risk pooling for rare-but-expensive events to the current dysfunctional system. And in the process also discusses some solutions to our current problems, such as Direct Primary Care.
(Read the full text of, "Why Health Insurance doesn't equal Health Care".)
Sunday, January 31, 2016
Adalja Lecture: Infectious Diseases and National Security
If you live in Colorado, you might be interested in this upcoming dinner lecture by Dr. Amesh Adalja: "Infectious Diseases and National Security" (March 12, 2016). I've already purchased my ticket!
Here's the announcement and the link to register:
Here's the announcement and the link to register:
Hungry Minds Speaker Series
Food for the body. Food for the mind.
Infectious Diseases and National SecurityThis talk will discuss the intersection of infectious disease emergencies and national security, with special attention to the speaker’s experiences with the ongoing Ebola and measles outbreaks as well as bioterrorism and biowarfare. The talk will also address the field of public health, delineating the proper role of government as well as the role of experts in shaping policy and engaging with the public.
A Dinner and Talk featuring
Dr Amesh Adalja
Senior Associate, UPMC Center for Health Security
Clinical Assistant Professor, Department of Critical Care Medicine
Clinical Assistant Professor, Department of Emergency Medicine
Adjunct Instructor, Division of Infectious Diseases, Department of Medicine University of Pittsburgh Medical Center
Saturday March 12, 2016
5:00 – 9:00 PM
C.B. & Potts
6575 S Greenwood Plaza Blvd
Englewood, CO 80111
303-770-1982
Agenda
5:00 PM: Cocktails, Dinner (Cash)
7:00 PM: Announcements
7:15 PM: Talk with Q/A
Cost
Advance General Admission: $35 per person ($40 after 3/4)
At the Door General Admission: $40 per person
Seating at Head Table with Speaker (space limited): $75 ($80 after 3/4)
Please Note: Purchase does not include dinner; order directly at event
Online reservations through March 9, or at the door.

Monday, January 25, 2016
Hsieh Forbes Column on New Year's Resolutions
My latest Forbes piece is now out: "Are You Struggling To Keep Those New Year's Resolutions?"
I discuss "temptation bundling" and other techniques to keep your New Year's Resolutions. And the fact that sometimes it's ok to just break them!

I discuss "temptation bundling" and other techniques to keep your New Year's Resolutions. And the fact that sometimes it's ok to just break them!
Monday, January 18, 2016
Armstrong on Quality
Dr. Richard Armstrong asks (and answers) a critical question: "Who Determines Quality in Health Care?"
A couple of excerpts:
Interestingly, the New York Times recently published a piece by Dr. Robert Wachter with a similar theme: "How Measurement Fails Doctors and Teachers". Wachter notes:
By the way, there is lots more good commentary on health policy at the Docs4PatientCare Foundation website by Armstrong (pictured below) and others.

A couple of excerpts:
[E]verywhere you turn someone is measuring something or surveying something or requiring the reporting of metrics. Patients are flooded with satisfaction surveys, doctors are inundated with pay for performance reporting requirements, physician quality reporting systems and, soon on the horizon from the federal government, the new Merit Based Incentive System. It’s enough to make your head spin. So, just exactly what is going on?...To concretize the issue, Dr. Armstrong poses an example of a patient "Jack" who needs a hernia repair. As a surgeon, Dr. Armstrong will work conscientiously to do his best by Jack. But Armstrong notes:
An estimated $3.5 trillion moves through our health care economy yearly. It should be no surprise that those who are purchasing health care would be concerned about the quality and value of their purchase. What is problematic is this…how do you measure it? Also, how can anyone be certain that they are measuring the “correct” things?
[T]he doctor should be working for the patient. But what happens when a third party, a private insurance company or the government is the purchaser of health care on behalf of the patient consumer? We are experiencing that today in America and the confusion is becoming mind numbing for both patients and doctors...As Dr. Armstrong notes, piling on more regulations onto a flawed system based on third-party payments won't fix the underlying problem. I recommend folks read the whole piece for themselves, as I'm only scratching the surface of his discussion.
Our “system” needs to focus clearly on producing high quality physicians and surgeons who understand why Jack and his family need quality care and that ultimately we are responsible to them, the patients.
It is no surprise that those who are paying for the services expect quality and value. Maybe it would be wise for all of us to re-evaluate how we are paying instead of expanding ever more complex, confusing and expensive “quality assurance” processes.
Interestingly, the New York Times recently published a piece by Dr. Robert Wachter with a similar theme: "How Measurement Fails Doctors and Teachers". Wachter notes:
Avedis Donabedian, a professor at the University of Michigan’s School of Public Health, was a towering figure in the field of quality measurement. He developed what is known as Donabedian’s triad, which states that quality can be measured by looking at outcomes (how the subjects fared), processes (what was done) and structures (how the work was organized). In 2000, shortly before he died, he was asked about his view of quality. What this hard-nosed scientist answered is shocking at first, then somehow seems obvious.“The secret of quality is love,” he said.Our businesslike efforts to measure and improve quality are now blocking the altruism, indeed the love, that motivates people to enter the helping professions. While we’re figuring out how to get better, we need to tread more lightly in assessing the work of the professionals who practice in our most human and sacred fields.
By the way, there is lots more good commentary on health policy at the Docs4PatientCare Foundation website by Armstrong (pictured below) and others.
Thursday, January 14, 2016
Edison Vs. American Board of Pediatrics
Dr. Megan Edison has written an "Open Letter to the American Board of Pediatrics".
Here is the opening:

Here is the opening:
Dear American Board of Pediatrics:She describes the numerous pointless "hoops" that pediatricians must jump through in order to maintain their certification (MOC), as well as questionable finances by the ABP leadership. In her words:
On December 17 2015, at 3:01 in the middle of my busy day seeing patients, I voluntarily gave up my American Board of Pediatrics certification. I thought I should write this letter, hopefully preempting any more threatening emails warning me that I must pay up or lose my certification. This was not mere oversight on my part. This was purposeful...
I am sad about giving up my ABP certification. I remember the elation I felt when I passed my boards after residency. I really felt like I had accomplished something and that my certificate represented my professional educational commitment to pediatric medicine. Now, after seeing the monster that board certification has ballooned into, I’m very happy to be off the MOC hamster wheel and no longer supporting a corrupt system that punishes very good doctors and pushes our most experienced pediatricians into early retirement.Dr. Edison also offers concrete reforms that the ABP can adopt. Let's hope the ABP chooses to listen to her.
Tuesday, January 5, 2016
Rising Interest in Health Care Ministries
The Wall Street Journal describes how "More People Turn to Faith-Based Groups for Health Coverage".
I very much like the idea of voluntary mutual-aid societies to share health costs. But some regulators don't. An except:
I very much like the idea of voluntary mutual-aid societies to share health costs. But some regulators don't. An except:
Ministry officials say they aren’t offering insurance, don’t guarantee claims will be paid, and don’t need to be regulated. The nonprofits are well managed, according to ministry officials, with third-party audits and a sterling history of sharing members’ claims.
Ministries generally don’t allow members to sue and require disagreements to be settled by arbitration and mediation.
Some ministries say they cost about 30% less than private insurance. Monthly payments, or sharing, may range from about $75 for a single person under age 30 to $500 or so for a family.
State regulators also say health ministries disrupt the insurance market because they tend to attract healthier consumers, siphoning them from commercial plans that can be left with sicker or older customers. Most ministries don’t always share bills for certain pre-existing conditions, whereas the ACA requires insurers to cover anyone regardless of their past or current medical history.
“They [ministries] have the potential to destabilize the market by drawing off the good risk,” said Mike Kreidler, Washington’s state insurance commissioner.
Monday, January 4, 2016
Doctors Vs. Bureaucrats
Dr. Marion Mass asks, "When will more Doctors stand up for their Patients and Themselves?"
An excerpt:
An excerpt:
Let’s get back to what really matters: the patient. At the moment I heard about not having crucial antibiotics for a sick infant, I snapped. I walked to the nearest phone and dialed the pharmacy, “Dr. Mass here. Why is patient x waiting for meds?”………(party line reply delivered)….”I see. You are going to mix up the antibiotics and get them to the ER in ten minutes. Otherwise, I will call the hospital CEO and tell him that I am going to tell the parents that their child is in danger because of hospital policy. I will not have some (un-publishable word) bureaucrat dictate my patient’s care. What? …Oh, thank you.” Coming clean to let you know how fun and liberating that moment was, as the ER staff stared at me in shock.Read the whole thing. (Via Dr. Megan Edison.)
I don’t wonder why more physicians don’t complain; it takes time. We are knee deep in CME, MOC, state and hospital mandates, insurance company fights, on and on. No wonder patients say we don’t take enough time with them. Furthermore, 80% of physicians are hospital-employed. Buck the system, lose a job. If you aren’t hospital-employed, you are bogged down keeping your indie practice alive for the sake of the patients you love...
Subscribe to:
Posts (Atom)