From CNN: "
One man's poop is another's medicine".
Donors who qualify can earn $40 per sample of "perfect poop", to be used for fecal transplantation to treat patients with C. difficile infection:
To donate, Eric had to pass a 109-point
clinical assessment. There is a laundry list of factors that would
disqualify a donor: obesity, illicit drug use, antibiotic use, travel to
regions with high risk of contracting diseases, even recent tattoos.
His stools and blood also had to clear a battery of laboratory
screenings to make sure he didn't have any infections.
After
all that screening, only 3% of prospective donors are healthy enough to
give. "I had no idea," he says about his poop. "It turns out that it's
fairly close to perfect."
And that,
unlike most people's poop, makes Eric's worth money. OpenBiome pays its
22 active donors $40 per sample. They're encouraged to donate often,
every day if they can. Eric has earned about $1,000.
Prospective donors are told, "It's easier to get into MIT and Harvard than it is to get enrolled as one of our donors."
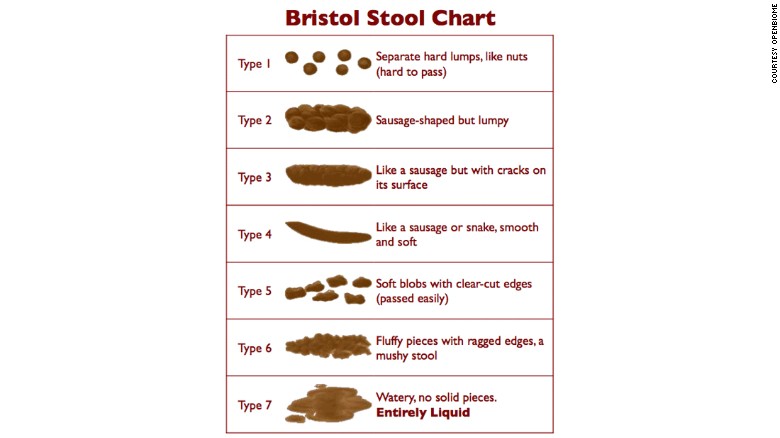
The poop also has to have the acceptable texture, either types 3, 4, or 5, on the Bristol Stool Chart: